grease ball
Daraxonrasib doubled survival in metastatic pancreatic cancer, and the ASCO auditorium stood up for 42 seconds.
May 31, 2026
A once-daily pill just doubled survival in metastatic pancreatic cancer, and the room that heard the data stood up and cheered for 42 seconds.
On May 31, at the plenary session of the 2026 American Society of Clinical Oncology Annual Meeting in Chicago, Brian M. Wolpin of the Dana-Farber Cancer Institute advanced to a slide showing that the drug daraxonrasib reduced the risk of death by 60% in patients with previously treated metastatic pancreatic cancer. The packed auditorium responded with a standing ovation, cheering, whistling, and applause that lasted 42 seconds, mid-presentation (Oncology News Central). Wolpin ad-libbed when the noise died down: "That time was not built into my talk" (Newsweek). The results were published the same day in the New England Journal of Medicine. Julie Gralow, chief medical officer of ASCO, called it "much more than a home run. I would actually say it's a grand slam" (Newsweek). Rachna Shroff, chief of hematology/oncology at the University of Arizona Cancer Center, said she had treated pancreatic cancer for 16 years and started crying in clinic when she saw the data (Newsweek).

RAS
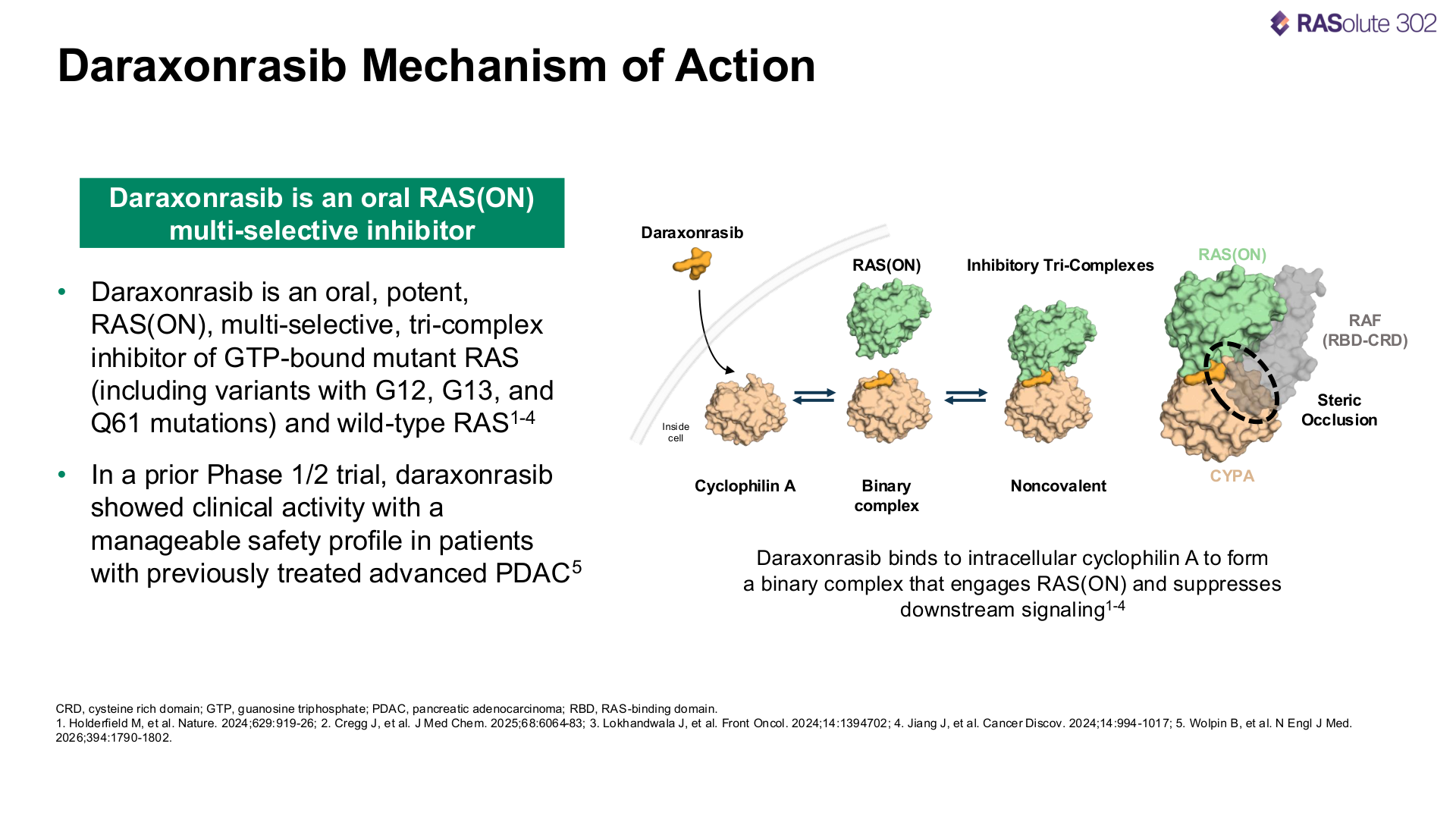
RAS proteins are a family of molecular switches inside human cells that regulate growth, division, and survival. They cycle between an active "on" state, bound to a molecule called GTP, and an inactive "off" state, bound to GDP. In healthy cells, RAS flips on briefly to relay a growth signal from the cell surface to the nucleus, then flips back off. The cycle is tightly controlled by two classes of regulatory proteins: GEFs (guanine nucleotide exchange factors), which activate RAS by loading it with GTP, and GAPs (GTPase-activating proteins), which deactivate it by accelerating the conversion of GTP back to GDP.
When the RAS gene is mutated, typically at positions G12, G13, or Q61, the protein loses its ability to return to the off state because GAPs can no longer trigger GTP hydrolysis, the switch gets stuck on, and the cell receives a continuous signal to divide. This is the central oncogenic driver in roughly 25 to 30% of all human cancers (PMC). In pancreatic ductal adenocarcinoma, the rate is over 90% (Bioquick News).
There are three RAS isoforms: KRAS, NRAS, and HRAS. KRAS is the most frequently mutated in solid tumors and accounts for the vast majority of RAS-driven pancreatic, colorectal, and non-small-cell lung cancers. The RAS oncogene was first identified in 1982, making it one of the earliest confirmed drivers of human cancer (PMC). Researchers spent the next four decades trying and failing to drug it. The protein is small, roughly spherical, and has an extremely high affinity for GTP, which leaves almost no accessible surface pocket for a conventional small molecule to bind. Shubham Pant of MD Anderson described the problem: "You can't stick anything to it. It just kind of slides off" (Managed Healthcare Executive), and the field called KRAS a greasy ball and "undruggable" for the better part of forty years.
Two cracks
The first crack came in 2013, when Kevan Shokat's lab at UCSF discovered that one specific KRAS mutation, G12C, briefly exposes a hidden pocket on the protein surface when the switch flips to the off position, and that a small molecule with a covalent acrylamide warhead could wedge into that pocket and lock the switch off (PMC). Amgen turned this into sotorasib (Lumakras), the first KRAS-targeting drug approved by the FDA, in 2021, for non-small-cell lung cancer. But sotorasib only targeted one mutation (G12C) in the inactive off state, and G12C is rare in pancreatic cancer, where the dominant mutations are G12D and G12V, which lack the exposed pocket Shokat found.

The second crack came from Gregory Verdine, a Harvard chemical biologist, serial biotech founder, and a pioneer of the field of chemical biology who coined the phrase "drugging the undruggable" (Wikipedia). Rather than trying to bind directly to the featureless surface of active KRAS, Verdine proposed using a molecular glue: a small molecule that first binds to cyclophilin A, a chaperone protein already present in the cell, creating a larger combined surface that can wrap around active KRAS and block it from signaling to its downstream effectors like RAF and PI3K (Lustgarten Foundation). The drug then drifts away and moves on to shut down another KRAS protein. Verdine has said: "I was inspired by nature to say: if nature has done this, can I reverse engineer it" (Lustgarten Foundation). He founded Warp Drive Bio in 2012 to build this platform.

In 2018, Revolution Medicines, a Redwood City oncology company led by physician-scientist Mark Goldsmith, acquired Warp Drive for approximately $88 million in stock (C&EN). The acquisition brought Verdine's molecular glue technology into a company already focused on the RAS pathway. Revolution narrowed its entire pipeline to what it calls "RAS-addicted" cancers and developed daraxonrasib (RMC-6236), an oral, multi-selective RAS(ON) tri-complex inhibitor that targets the active GTP-bound state of mutant and wild-type RAS across G12, G13, Q61, and other variants (Revolution Medicines), where first-generation drugs hit one mutation in the off state and daraxonrasib hits multiple mutations in the on state.
The trial
The Phase 3 trial, RASolute 302 (ClinicalTrials.gov NCT06625320), enrolled 500 patients with previously treated metastatic pancreatic cancer across 59 sites in six countries, randomized to daraxonrasib (n=248) or investigator's choice of four chemotherapy regimens (n=252). The trial was funded by Revolution Medicines (Nasdaq: RVMD). Topline results were released April 13, 2026 (Revolution Medicines). Detailed data were presented at the ASCO plenary on May 31 and published simultaneously in the NEJM.
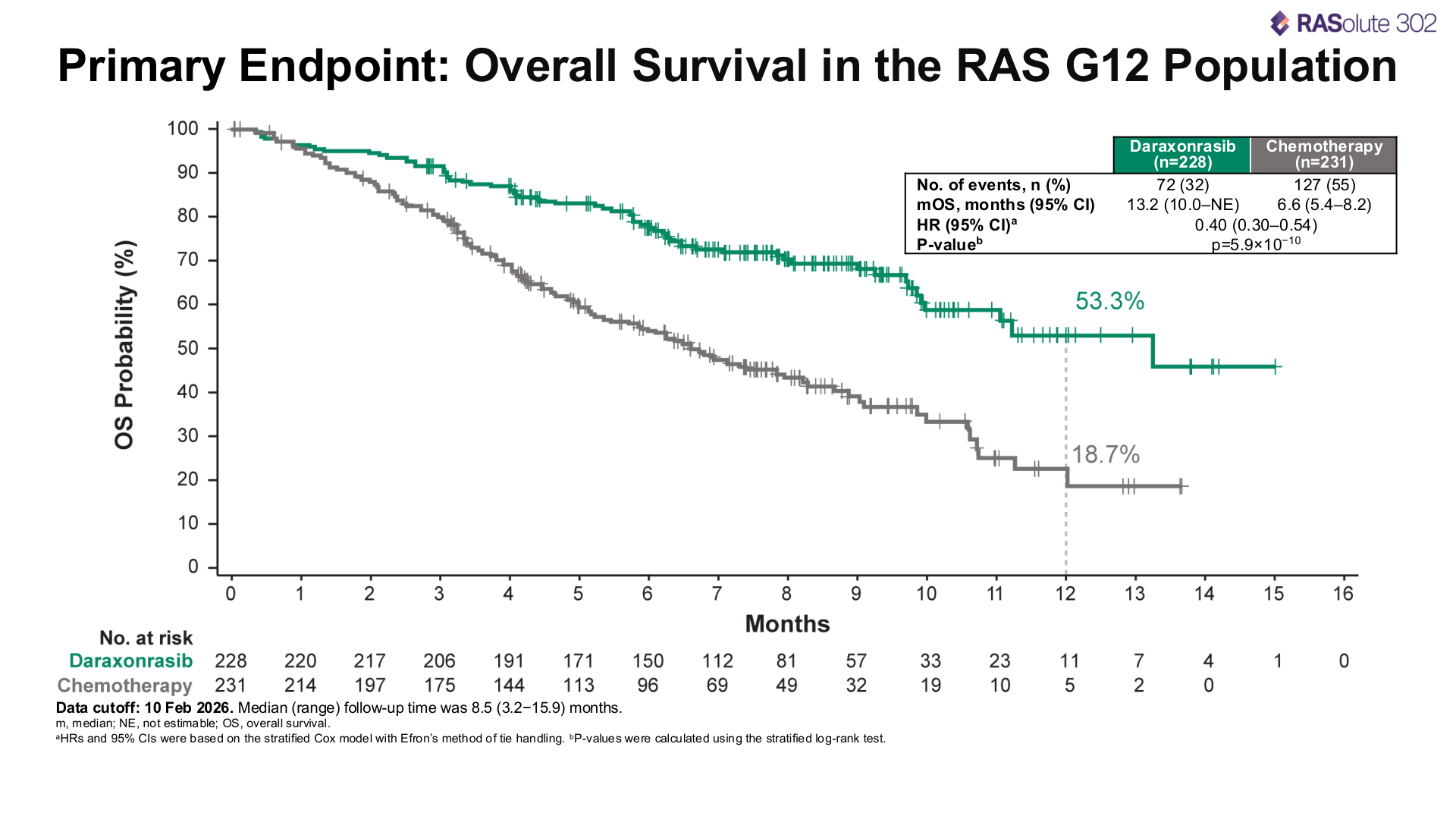
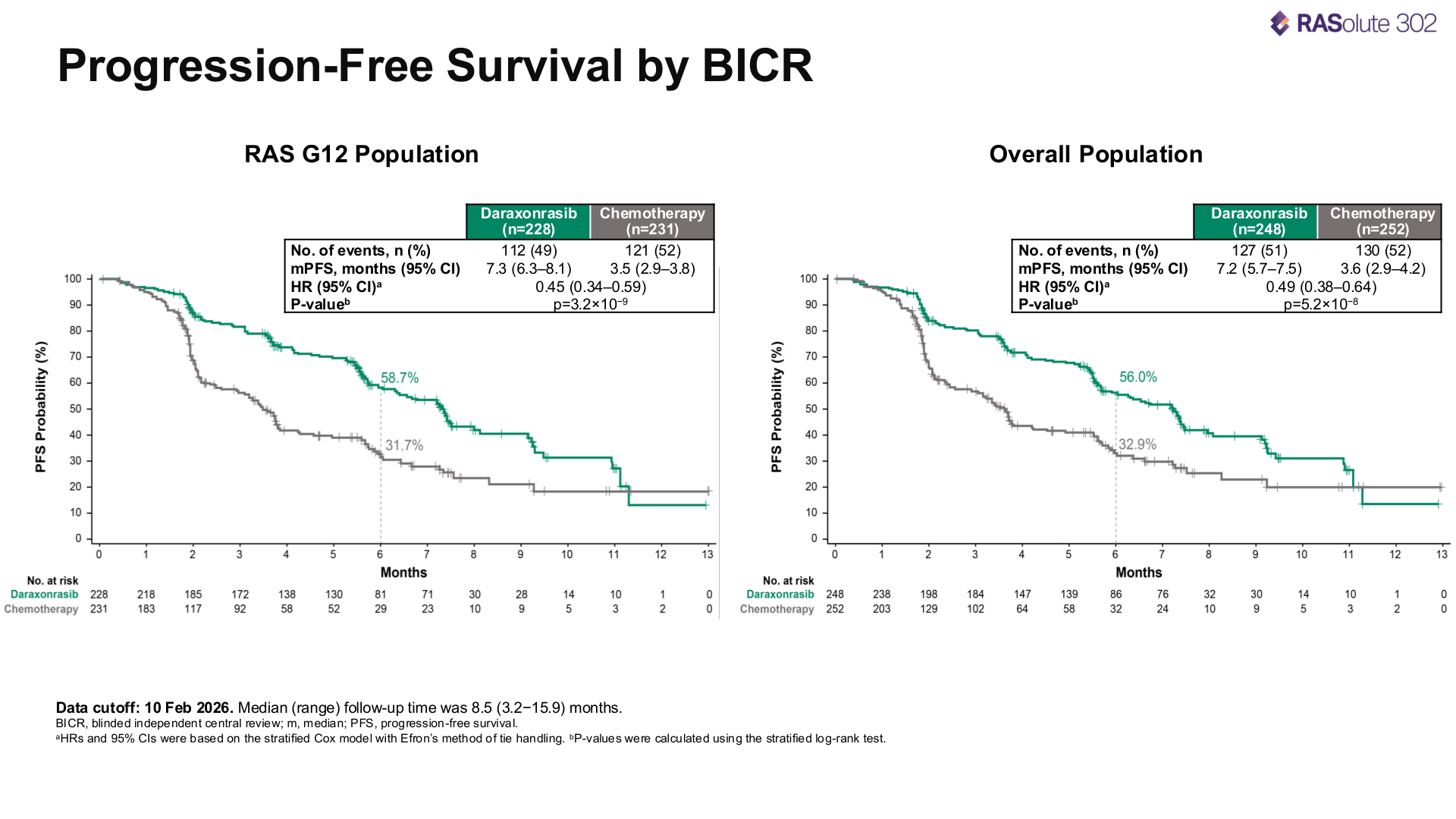
At a median follow-up of 8.5 months, in the RAS G12 population (228 daraxonrasib, 231 chemo), median overall survival was 13.2 months versus 6.6 months (HR 0.40, p < 0.0001). In the full intent-to-treat population it was 13.2 months versus 6.7 months. The twelve-month overall survival rate was 53.3% versus 18.7%, median progression-free survival was 7.3 months versus 3.5 months, and the objective response rate was 33.2% versus 11.8% (ASCO Post, Let's Win).
Grade 3 or higher adverse events occurred in 43.6% of daraxonrasib patients versus 57.5% on chemotherapy. Treatment discontinuation due to adverse events was 1.2% versus 11.2%. The most common side effects leading to dose reduction were rash and oral sores, and one patient in the daraxonrasib arm died from treatment-related pneumonia (ASCO Post, Managed Healthcare Executive).
The survival benefit held across patients with G12 mutations, other RAS mutations, and patients with no identified RAS mutation, and the trial met all primary and key secondary endpoints, the first Phase 3 trial in any line of therapy for metastatic pancreatic cancer to report a median overall survival exceeding one year (Revolution Medicines ASCO release).
Revolution
Revolution Medicines was founded in 2014 by Goldsmith, a physician-scientist out of Third Rock Ventures. The company went public in February 2020 at $20 per share, raising $238 million, and has since narrowed its focus to RAS-addicted cancers (FinancialContent). In mid-2025, Revolution signed a $2 billion deal with Royalty Pharma to finance the push toward commercialization. In October 2025, daraxonrasib received a Commissioner's National Priority Voucher from the FDA, which accelerates review (Revolution Medicines). Revolution has four clinical-stage RAS(ON) inhibitors with differentiated profiles: daraxonrasib (multi-selective), elironrasib (G12C-selective), zoldonrasib (G12D-selective), and RMC-5127 (G12V-selective), all built on the same tri-complex/cyclophilin A platform (Revolution Medicines), and daraxonrasib's success is early validation for the platform as a whole.
Goldsmith: "This class of inhibitors reflects more than 15 years of investment in groundbreaking scientific research, including creative work from Warp Drive Bio, acquired by Revolution Medicines in 2018, which established the initial technology foundation" (Revolution Medicines). Verdine, now co-founder of Parabilis Medicines, on the broader class: "We have people who have been on this drug for three years. It is kicking ass" (Nature).
What comes next
Revolution is testing daraxonrasib as a first-line treatment for metastatic pancreatic cancer, in combination with chemotherapy and other agents (PanCAN). The company intends to file a New Drug Application with the FDA under the Priority Voucher. Expanded access is already open for eligible patients through their treating physicians (PanCAN). The primary competitor is Eli Lilly, advancing olomorasib through its own RAS program but trailing Revolution by roughly 12 to 18 months in the pancreatic indication (FinancialContent). Merck acquisition speculation circled Revolution in January 2026 and has not been resolved (The Pharma Letter).
Resistance will likely emerge, and researchers have already identified mechanisms including KRAS switch-region mutations and bypass through BRAF and other pathways, so duration of response will determine whether daraxonrasib is a temporary reprieve or a lasting shift in a disease where the protein that drives 90% of cases was considered untouchable for forty years and a daily pill has now doubled survival with fewer side effects than chemo. Eileen O'Reilly of Memorial Sloan Kettering: "This drug is potentially going to be a landmark shift in how we treat pancreatic cancer" (MSK). Anna Berkenblit, chief scientific officer of PanCAN: "The most significant advance we have ever seen in pancreatic cancer" (PanCAN).